Homeopathic Management of Developmental Delay: Dr. S.G Biju - The Importance of Early Stimulation and Parental Awareness
Abstract
While treating developmental delays through homeopathy, medication alone is often insufficient. Appropriate sensory, motor, emotional, and social stimulation plays a crucial complementary role in optimizing a child’s development. Equally important is educating parents so that early warning signs are recognized and timely interventions are initiated. In this article, I share my clinical experience in identifying developmental risks, anticipating delays, and integrating homeopathic treatment with structured stimulation strategies.
Introduction
Developmental delay is a multifactorial condition influenced by genetic, biological, environmental, and antenatal factors. Early identification and intervention significantly improves outcomes. A physician treating children homoeopathically must anticipate developmental, behavioural, and learning difficulties, even before obvious delays become evident. Proper stimulation tailored to each developmental stage is essential alongside individualized homeopathic prescriptions.
Risk Categories for Developmental Deficits
Developmental deficits may arise from the following risk categories:
1. Established Risk
- Maternal illness during the first trimester of gestation
- Teratogenic effects of certain drugs
- Exposure to X-rays during the second half of the menstrual cycle
- Chromosomal anomalies
2. Environmental Risk
- Lack of sensory, emotional, and social stimulation
3. Biological Risk
- Low birth weight (below 2.5 kg)
- Premature birth
- Asphyxia neonatorum
- Hyperbilirubinemia
- Hypoglycemia (often associated with gestational diabetes mellitus)
- Neonatal convulsions
- Intrauterine infections
- Septicemia
4. No Apparent Risk
- Children may still present developmental delays despite no obvious identifiable risk factors
Conditions Requiring Anticipation of Developmental Problems
A physician should be vigilant for developmental, behavioral, or learning abnormalities in children with the following history:
1. Delayed conception
2. Repeated abortions
3. Excessive vomiting during the first trimester
4. Low birth weight
5. Neonatal jaundice
6. Hypoglycemia
7. Neonatal convulsions treated allopathically
8. Maternal psychiatric illness
Nature of Delivery and Miasmatic Predisposition
The mode and circumstances of delivery may indicate the child’s dominant miasmatic tendency:
- Normal delivery – Psoric
- Delayed, prolonged, or cesarean delivery – Sycotic
- After multiple abortions or maternal death – Syphilitic
- Preterm delivery – Tubercular
- Severe complications requiring surgery but ending in normal delivery – Cancerous
Milestone Development in Children
Several tools are available for assessing developmental delays, including:
- Developmental Assessment for Indian Infants (DAII)
- Amiel-Tison passive angle method
- Trivandrum Development Screening Chart (TDSC)
- CDC grading for motor milestones
- Denver Developmental Screening Test
- Neurological evaluation
In South India, the Trivandrum Development Screening Chart (TDSC) is widely accepted.
Early Social and Visual Milestones
Social Smile (5–45 Days)
A social smile should develop between 5 and 45 days.
Stimulation:
The mother should smile at the child, maintaining eye contact while the child is awake.
Clinical Tip:
If social smile does not appear by 10 days and is associated with umbilical bleeding, Abrotanum 30 may be considered.
Response to Mother (By 45 Days)
By 45 days, the child should show excitement when transferred to the mother.
- Stimulation: The mother should actively engage and express enthusiasm.
- Remedies: Medorrhinum 10M, Baryta carbonica 30
Visual Tracking and Eye Contact (5–50 Days)

The child should visually follow a moving object and develop eye-to-eye contact.


Clinical Approach:
- If absent, rule out visual impairment.
- If vision is normal, consider reduced brain response (e.g., autism spectrum).
Stimulation:
High-contrast visual images and pictures placed near the child’s interaction area.
Miasmatic Consideration:
Often syco-syphilitic; treat with appropriate genetic nosodes such as Medorrhinum, Syphilinum, Tuberculinum, Carcinosinum, or Psorinum.
Head Holding (40–150 Days)
The child should hold the head steadily by 120 days.
Stimulation Techniques
- Support the child through the axilla and cervical region
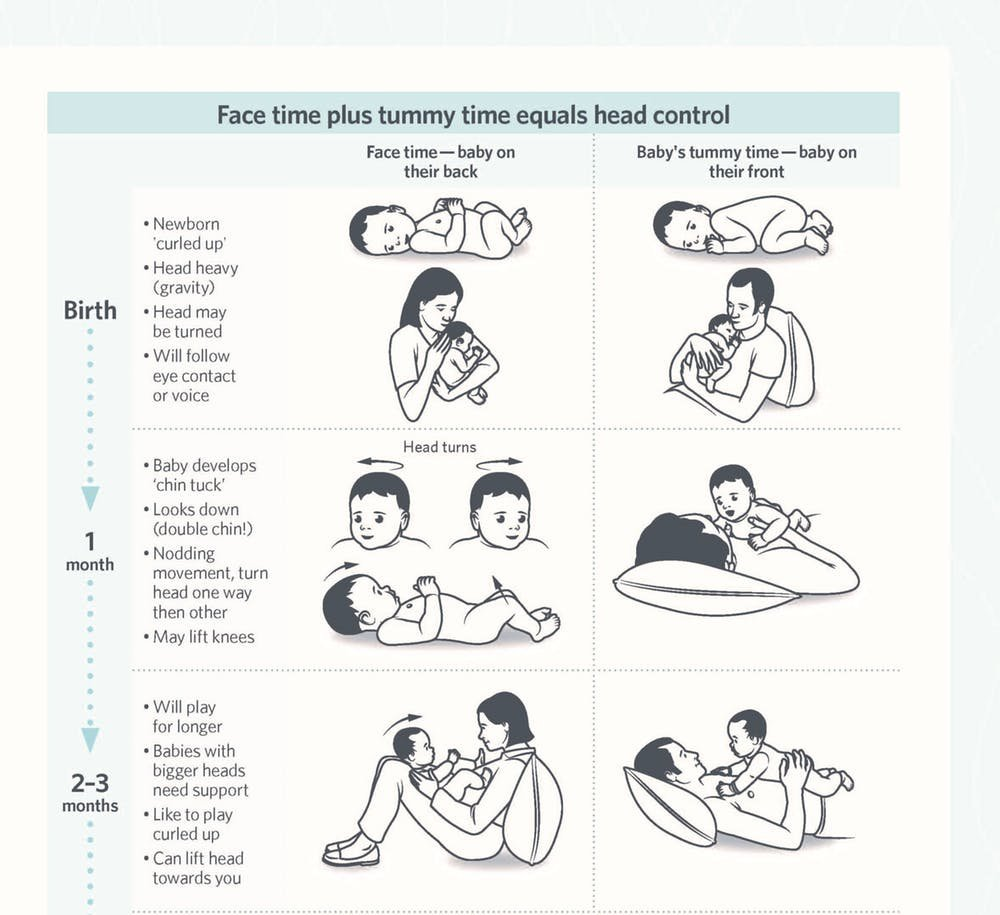
- Massage the spine while the child is seated on the lap

- Use colourful or sound-producing toys above head level
- For joint instability, seat the child on bent knees and perform cycling movements
Treatment
- Joint instability: Silicea 200
- Lean, premature infants: Calcarea phosphorica 30
- Obese infants: Calcarea carbonica 30
- Maternal thyroid disorders during pregnancy: Parathyroidinum 30, Pituitary 30
Rolling Over (3–6 Months)
The child should roll from back to abdomen.
Stimulation:
- Gently guide the child’s limbs to assist rolling
- Encourage twisting movements
- Lift gently using crossed fingers under the chest
Clinical Prescriptions:
- Obese child with maternal emotional shock: Natrum muriaticum 200
- Maternal steroid use: Sepia 200
- History of difficult labor: Medorrhinum 10M
Prone Position and Auditory Response (3–5 Months)
The child lying prone should turn the head toward sound.
Stimulation:
- Place the child on the stomach
- Attract attention with bells, rattles, toys, and colorful objects
Treatment principles remain similar to those for delayed head holding.
Bilateral Coordination (3–4 Months)
The child should bring hands or feet to the mouth, reflecting hemispheric coordination.
Stimulation:
Guide the child’s hands gently to the mouth.
Remedies in Neural Deficits:
Zincum metallicum, Cuprum metallicum, Hypericum, Opium, Argentum nitricum
Object Transfer (4–7 Months)
The child should transfer objects from one hand to the other.
Stimulation:
Teach the child to hold and transfer toys between hands.
Treatment Options:
- With head complaints: Belladonna, Aconitum
- With generalized incoordination: Agaricus, Alumina, Calcarea phosphorica, Causticum, Conium, Cuprum met., Fluoric acid, Graphites, Kali bromatum, Lachesis
Sitting, Standing, and Walking Milestones
Sitting (5½–10 Months)
- Stimulation: Assist sitting with support at the waist
- Remedies: Baryta carb, Calc phos, Calc carb, Phosphorus, Nat mur, Silicea, Tuberculinum, Medorrhinum 10M
Standing with Support (6–11 Months)
- Stimulation: Encourage standing using furniture
- Remedies: Calc carb, Thuja, Calc phos, Medorrhinum, Tuberculinum, Opium
Walking with Support (7–12 Months)
- Stimulation: Child’s feet placed over mother’s feet while walking
- Remedy: Calcarea phosphorica
Independent Walking (9–16 Months)
- Stimulation: Use walkers cautiously



Speech and Social Interaction
Speech Development (9–17 Months)
The child should speak one or two words.
Stimulation:
Face-to-face interaction with slow, clear, expressive speech.
Remedies:
Natrum muriaticum, Calcarea phosphorica, Medorrhinum 10M, Thuja, Tuberculinum
Advanced Motor Skills
- Walking backward (11–18 months): Encourage through play
- Climbing stairs (12–20 months): Assist initially, then encourage independence
- Pointing body parts (15–24 months): Repeated imitation and play-based learning
Developmental delays require a holistic approach. Homeopathic medicines, when combined with timely stimulation and parental education, can significantly enhance a child’s developmental trajectory. Awareness, anticipation, and early intervention remain the cornerstones of successful management.
Dr S G Biju, BHMS, MD (Hom.)
The Homoeopathic Multispeciality Hospital
Palace Road, Changanassery – 1
🌐 www.drbijuonline.com
📧 drbijugnair@gmail.com
📞 9447128799 (WhatsApp only)